
EXPERIMENT 1: The Burn Study
EXPERIMENT 1
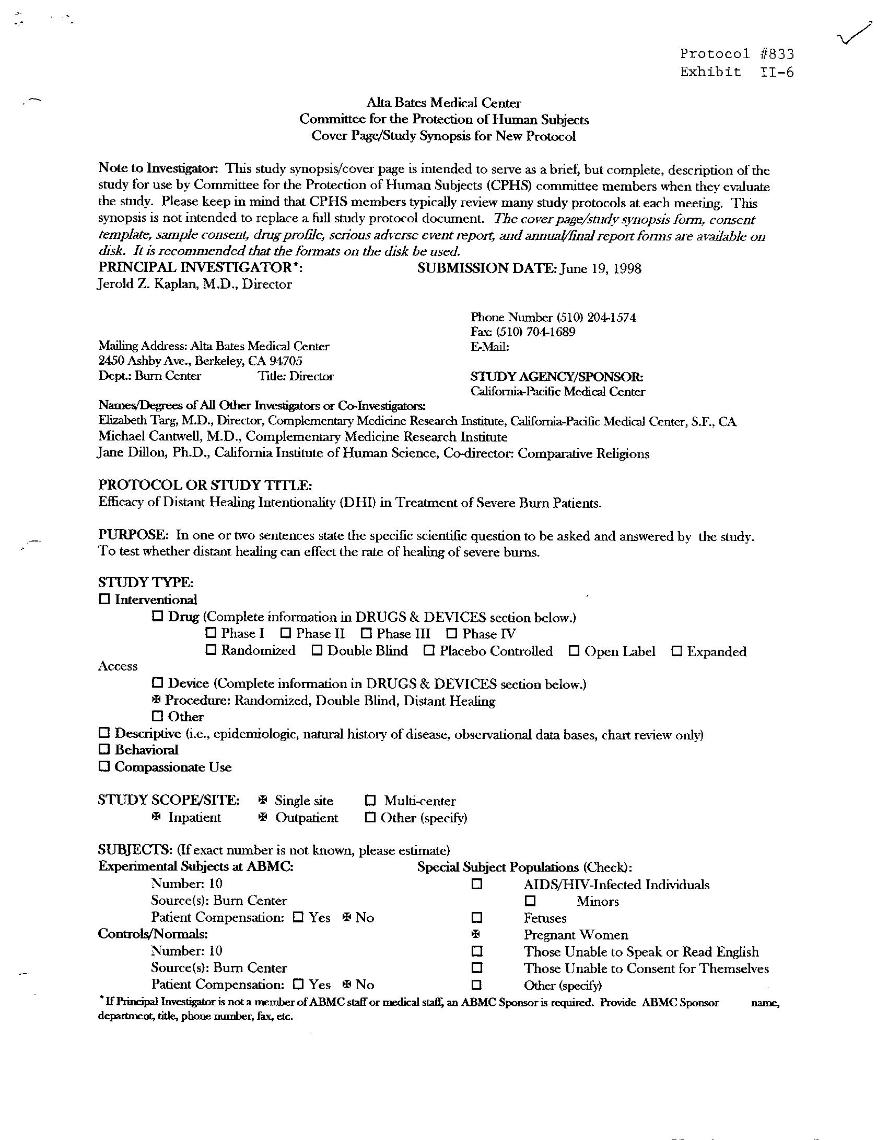
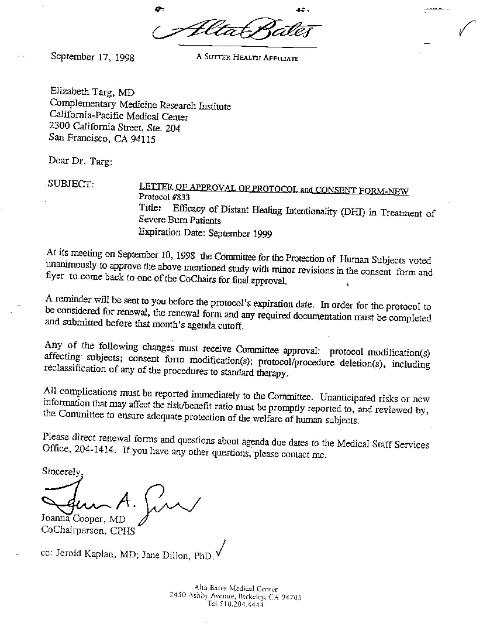
PROTOCOL Conduct a six-month double-blind clinical trial to document the immediate effect of Distant Subliminal Neuro-Bypass (DSNB) processing (specific use of SDI) on a specified number of subjects suffering from severe fire burn injuries within the first hours of exposure by using only the victim's name, photograph, and place and date of birth as coordinates, so that results are visible, clearly understandable, incontrovertible, reproducible and absolutely not currently part of any existing scientific paradigm, to ensure that the experiments truly validate the existence of "transcendental forces," "a higher power" and another "reality," which are as yet unacknowledged by reductionist science. HYPOTHESIS 2. There are no risks to subjects in the study and no interference with normal medical procedures. 3. Subjects in the treatment group are less likely to die than those in the control group. When someone who is bound to die a certain death within a few hours of fire exposure can be subliminally (unknown by the subject) convinced not to, and when the SDI operation can thus violate all known laws of physics and of medicine, and when we can reproduce the same phenomenon on thousands of cases with an extraordinary rate of 100% success, the value, efficacy, reliability, and repeatability of the revolutionary science of Subliminal Influentiality is validated with incontrovertible certainty and the existence of a higher power and transcendental bio-forces are documented and accessible for scientific investigation. SPECIFIC DESIGN CRITERIA Clinical Trials of SDI on subjects suffering from severe Fire Burn injuries were conducted in two California Burn Units. The double-blind Burn Study is a set of clinical trials of SDI DSNB processing of people with severe third-degree burns conducted at two prestigious Burn Centers in California. The purpose is to document the results of SDI technology in an area of emergency medical science that doctors cannot treat. According to medical doctors, severe third-degree burns cannot heal, there can be no reepithelization of the skin. If there could be, the wound would be called a severe second-degree burn. When severe third degree burn shows any reepithelization of skin, from any treatment, those results document that something impossible has happened. Project Investigators: Dr. Elizabeth Targ, MD, Research Director, CPMC Dr. Jerold Kaplan, MD, Director of Surgery, Alta Bates Hospital Dr. Michael Cantwell, MD, University of San Francisco, CA Dr. Jane Dillon, PhD, University of California San Diego Approval from Alta Bates Human Subjects Review Board for a six-month clinical trial was received on September 17, 1998. Principal Investigator Dr. Elizabeth Targ summarized the Burn Study design proposal using the language of her well-known research on Distant Healing Intentionality (DHI) and received an encouraging endorsement from the renowned medical doctor Dr. Larry Dossey, executive editor of Alternative Therapies and co-chair of the panel on Mind/Body Interventions of the National Institutes of Health. (See below) Principal Investigator Dr. Jerold Kaplan submitted the formal Burn Study proposal to the Alta Bates Medical Center Review Board on June 19, 1998, which was accepted by Dr. Elizabeth Targ on September 17, 1998. (See below) |
Dr. Savage explains: "Very complicated psychological and cultural factors of physiological self-destruction are at play in cases of severe fire exposure traumas. There are strong scientific elements which suggest that it is not really, nor only, the exposure to fire that kills people: Rather, it is the subjects' own perception of what they believe to be a fatal accident that triggers most of the immune traumatic processes usually observed in cases of severe burn-related injuries. The dramatic influence of the mind on the body has been scientifically documented. According to their own cultural or psychological makeup, when people are facing the same kind of injury or disease, some of them go to a lethal conclusion, whereas some of them recover. The well-known "placebo effect" has shown with extreme clarity that the subjective perception of a person on his/her own wound or sickness affects immensely the self-healing processes. Some people are known to walk and dance in the fire for a protracted period of time without being affected in the slightest, while their clothes go immediately ablaze. An altered state of consciousness related to the situation of mystical trances accounts for this major discrepancy. It is because they can bypass their own perception of the reality that those subjects sort of "mindhack" themselves: In doing so, they are capable of transcending our cultural perception of fire and to evade temporarily our paradigmatic reality in which flame exposure logically entails disastrous traumatic results. |



Project Investigators: Dr. Matt Young, MD (Burn Center) Dr. Jane Dillon, PhD (University of California) Dr. Richard Grossman, MD (Grossman Burn Center) Pilot Burn Study authorization received from Burn Center founder Dr. Richard Grossman, MD, for a six-month study, October 1998 - March 1999. While waiting for the completion of the long-term formal double-blind study at Alta Bates Hospital, Dr. Jane Dillon and Dr. Matt Young (authorized by Dr. Richard Grossman and supervised by Dr. Peter Grossman) documented the clinical progress of five subjects who received DSNB processing (Treatment Group), and five subjects who did not receive DSNB processing (Control Group) during the Pilot Study. All ten subjects in the study received the usual course of treatment from the burn center. Project investigator Dr. Young is a pediatrician and as it turned out all the ten subjects involved in the study were children. The five children in the Treatment Group were cases that Dr. Young or Burn Unit staff informed Dr. Dillon of as soon as they were admitted to the burn unit. The children in the Control Group (not treated by DSNB processing) were the first five children who were admitted to the Burn Unit during the study, but that Burn Unit staff did not contact Dr. Dillon about when admitted. (Two of those children subsequently died at the Burn center). Dr. Young observed and reported on the cases of all ten children in the study. Dr. Dillon was invited to personally observe the results of three of the children in the Treatment Group. The primary hypotheses of this Pilot Burn Study were, a) subjects in the treatment group are more likely to show reepithelization (natural healing) of skin than those in the control group, and b) subjects in the treatment group are less likely to die than those in the control group. Although further tests are required for statistical significance, utilizing many more than ten cases, we can at this point say quite conclusively that the historic Pilot Burn Study documents 100% positive outcomes. RESULTS The results of the SDI processing on the children in the treatment group, as compared with the children in the control group, were a shocking and unprecedented 100% success. CASE DESCRIPTIONS Case #TG9 is a three-year old girl (DW) who fell into scalding bathwater with her clothes on, burning 65% of her body (all except her head). This child received emergency DSNB (SDI) processing within three hours after the accident, while she was en route from UCLA emergency to the Grossman Burn Center. By the time she arrived, she was unusually calm. She remained calm, needing very little pain medication for the rest of her stay, throughout which most of the third-degree burned areas showed reepithelization of skin. (As noted, several small areas on wrists, hands, and thigh received minor grafting). Two days after her release from the Burn Center, the child returned for a follow-up visit dressed in a new dress, red winter coat and leggings. Upon examination of her skin, there continued to be rapid healing and no discomfort for the child. These results, merely five weeks after an accident in which a child this size could have been expected to die, astounded this girl's parents, as well as Dr. Young and the Burn Unit staff. Case #TG10 is a nine-year old boy (AC) who was severely burned by a bomb placed in a gopher hole that exploded in his own face. This boy's face was burned from the nose up, with eyebrows burned off and eyes swollen shut. He received DSNB (SDI) processing approximately nineteen hours after the accident. Within four days, his condition was so well improved that he went home the following day, seeing with open eyes, and his forehead looking as if it had only been mildly scraped on the sidewalk. The remarkable healing of skin amazed both his parents and the medical staff who took care of him. DISCUSSION of third-degree burns. According to medical definition, third-degree burns do not heal. In each case in the treatment group, large sections of the patient's burned skin were diagnosed by one to three medical doctors as third-degree. The records show that over a period of time (ranging from 1 to 5 weeks), most of the third-degree burned areas healed (showed reepithelization of skin) and the children went home with little or no need for grafting. We have been told by every medical authority we contacted that such dramatic results are, in fact, unheard of in medical research. Third-degree burns, by definition, are not known to heal. If a burned area is diagnosed as severe, but with a possibility of reepithelization of skin, it is called a second-degree burn. All the children in the treatment group showed significant reepithelization of skin in areas diagnosed by one to three medical doctors as third- degree burn. All the children in the treatment group received exactly the same cares as those in the control group (as all previously treated burns at the burn center). The only difference was the additional application of Philip Savage's DSNB (SDI) subliminal technology to children in the treatment group. Since these five children received exactly the same cares from the burn center as did other children treated in the past, there is no other explanation for the enormous discrepancies in the normal course of outcomes for these five cases. In the control group of children who did not receive Dr. Savage's DSNB processing (because hospital staff did NOT call the research team for help), two children died within a week, and the three who were not in critical condition showed no reepithelization of skin and instead received normal grafting of their third-degree wounds. children who were unaware of any distant Subliminal Processing. The possibility of placebo or psycho-social expectancy (i.e., effect of belief), although not known to ever affect medical healing of third-degree burns, is thus eliminated. Nor did these children ever exhibit any behavior associated with hypnosis. If anything, the behavior of these children was described by medical staff as more alert, more vital, and more willful than other children treated at the burn center. Dr. Savage's 30-minute protocol where outcomes are expected by the researchers to be even more dramatic. Implementation of Philip Savage's SDI technology only on FIRE-related burns within the first minutes of exposure will reduce the risk of failure to zero, with 100% guarantee of complete healing. Strict respect of Dr. Savage's protocol also enables more subjects to be treated each day without affecting the potency of DSNB processing (with the possibility of 100% successful treatment of many thousands of burn victims per day when global emergency teams are trained in the DSNB processing). Experiment 1 on Subliminal Influence distant treatment of severely burned hospitalized children with 100% successful results in the Treatment Group (and NO change in the normal course of events in the Control Group) proves that something very unusual (considered "impossible" by medical science) is going on that doctors and hospital staff don't know how to do, nor even know exists. Such proof of the truth (experical facts) that some kind of "unknown higher power" exists that is accessible and capable of bringing observable, verifiable and replicable scientific results, without a "placebo effect" and with 100% success rate, is until now unheard of in medical science. to others, 2) Make the DSNB technology available, nationally and internationally, in additional testing sites, and 3) Contribute to the understanding of this new science of Subliminal Influentiality that has the potential to eradicate the pain, suffering and death from burns throughout the world. FOOTNOTES 1. TG9 CASE, (DW): Twenty years after her life-threatening burn injury, one of the children in the Treatment Group of the Pilot Burn Study (DW) now has a website of her own discussing and describing her remarkable experience when she was 3 years old. Still unaware of what actually happened and that she received a "special SDI treatment" from a distance, DW's personal story is fascinating documentation of the efficacy and non-placebo effects of Dr. Savage's SDI technology on severe life-threatening burns. 2. GHANA CASE, (ADELAIDE): Although not part of the 1998 Historic Burn Study with its ground-breaking results, and called in many hours after severe fire injuries were sustained by the burned children, the following burn case described by a former nurse gives an astonishing visual demonstration of what Dr. Savage's SDI (DSNB) processing can do in emergency situations where people are burned by fire. Immediate life-saving results like these could also have been recorded at the Grossman Burn Center had the Burn Unit staff contacted the SDI research team when the two young boys, CG1 and CG2 above, were severely burned by fire and instead died, without receiving Dr. Savage's immediate DSNB processing. (Unfortunately, external human errors and complexities at the Burn Center, outside of the SDI/DSNB Protocol, produced these two disastrous life-ending results that could have so easily been avoided.) Mary Badham (former burn nurse) recalls the story of Ghana Girl Adelaide "There was a little girl in Ghana whose house caught on fire. There were 3 children... and she lost tissue almost across her whole abdomen and down the front of her legs. Now, burns if it’s much larger than a quarter, they usually have to graft, skin graft – that entails using skin from another part of the body and putting it on there or using – if that’s not available, they have grown skin that they can use and various other methods but this takes weeks, months, years to do. Most of the time when you have burns over 40% of the bodies, the patients very often don’t make it. This child had been taken to hospital and this child healed. We have photographs of her now and it’s just amazing. Normally when you get burned, it takes all the pigment out of the skin. She didn’t even lose the pigment on the skin, it grew back of its own accord. I just thank God every day that this is an ability that we have now." |
CONTROL GROUP DATA Did not receive SDI processing Case #CG1: Seven-year old boy ("ANN") 12/30/98 Third degree fire burn to face, trunk, limbs. 12/30/98 Diagnosed critical condition at burn center. Usual course of treatment. Hospital staff did not call for SDI processing.. 1/04/99 Died at burn center. Case #CG2: Fifteen-year old boy ("BNN") 12/30/98 Third degree fire burn to face, trunk, limbs. 12/30/98 Diagnosed critical condition at burn center. Usual course of treatment. Hospital staff did not call for SDI processing. 1/08/99 Died at burn center. Case #CG3: Small child ("CLN") 1/5/99 Third-degree scald burn to left upper arm (tea). 1/5/99 Diagnosed at burn center. Usual course of treatment. Hospital staff did not call for SDI processing. ------- Went home with grafting. Case #CG5: Six-month old boy ("KV") 1/12/99 Third-degree scald burn to trunk and limbs (coffee). 1/12/99 Diagnosed at burn center. Usual course of treatment. Hospital staff did not call for SDI processing. ------- Went home with grafting. Case #CG7: Ten-year old boy ("AB") 1/14/99 Third degree fireworks burn to lower left leg/foot. 1/14/99 Diagnosed at burn center. Usual course of treatment. Hospital staff did not call for SDI processing. ------- Went home with grafting. |
TREATMENT GROUP DATA Received SDI processing Case #TG4: Three-year old girl (CLC) 1/10/99 5:00 pm On route to burn center, third degree scald burn. 1/10/99 6:00 pm Diagnosed at burn center, third degree to trunk and and perineum. 1/11/99 10:00 am Subliminal processing (SDI). 1/28.99 Doing great. Went home in 17 days. No grafting. Case #TG6: Eight-month old girl (AN) 1/13/99 6:00 pm On route to burn center, 30% of body scald burn. 1/13/99 7:50 pm Diagnosed at burn center, third degree. Critical condition 1/14/99 11:30 am Subliminal processing (SDI). 1/28/99 Doing great. Last surgery. Going home. 2/3/99 Went home in 21 days. No grafting. Case #TG8: One-year old girl (BR) 1/28/99 10:30 am On route to burn center, 30% of body scald burn. 1/28/99 2:30 pm Diagnosed at burn center, third degree. Critical Condition. 1/28/99 3:00 pm Subliminal processing (SDI). 2/1/99 First chance to see extent of wounds in surgery. Third degree burns turned into 2nd degree and are healing. Only tops of feet grafted. 2/5/99 In surgery, there was no further grafting. Burns are healing. Doing very well. 2/10/99 Went home in 15 days. All healed. No grafting, except minor spots on tops of feet. Case #TG9: Three-year old girl (DW) 2/3/99 4:30 pm On route to burn center, 65% of body scald burn. 2/3/99 7:30 pm Subliminal processing (SDI) on route to burn center. 2/3/99 8:15 pm Diagnosed at burn center, third degree. Critical condition, yet very calm. 2/10/99 Still calm, little need for pain medication. Risk of infection. Limbs are healing. Overall good. 2/16/99 Still doing well, overall. No infection. 3/1/99 Off critical side. Third degree burns are healing. Minor grafting of hands, wrists and spot on thigh. 3/10/99 Went home in 35 days. All healing. No grafting, except minor spots on wrists, hands, thigh. Case #TG10: Nine-year old boy (AC) 3/7/99 3:00 pm On way to burn center, explosion burn to face, third degree. 3/7/99 8:45 pm. Diagnosed at burn center. Eyebrows gone, eyes swollen shut. 3/8/99 10:00 am Subliminal processing (SDI) 3/12/99 Doing great. Eyes half open. Forehead looks scraped. All healing. Going home this week. 3/13/99 Went home in 6 days. No grafting. |
areas diagnosed with deep and severe third degree burn.
group. 2. In all five cases in the treatment group, the children not only survived their critical condition, but went home strong, with healing skin.
week of admission to the burn center; and the other three children who were not in critical condition eventually went home with normal grafting of third-degree burn areas. 3. In all five cases in the treatment group, there was a subjectively noticeable and unusual lack of infection, lack of pain and discomfort, vitalization of will, and maintenance of calm throughout each subject's stay at the burn clinic. |
MEDICAL DOCTOR'S REPORT OF GHANA GIRL ADELAIDE BURNED BY FIRE Six-year-old Adelaide was severely burned in a 2010 house fire, and fully recovered after Dr. Philip Savage, a.k.a.the FireBurnDoctor, intervened from a distance. On August 6, 2010, during the night, the family's house caught fire (due to an electrical fault) with three children inside. Adelaide and her brother and sister had severe burn injuries. Of the three children, the situation of Adelaide was most severe and doctors feared for her life when she was brought to the hospital. The next day, a local assemblyman in Ghana called Dr. Savage's team for help. The children were treated immediately by Dr. Savage and his remote SDI intervention method for burns (DSNB). As a result, all three children experienced accelerated recovery, including Adelaide, whom doctors expected to die. In March 2011, Dr. Savage's team received the following shocking "BEFORE" and “AFTER” photos, showing Adelaide's full recovery and natural restoration (healing) of skin in her same pigment. |
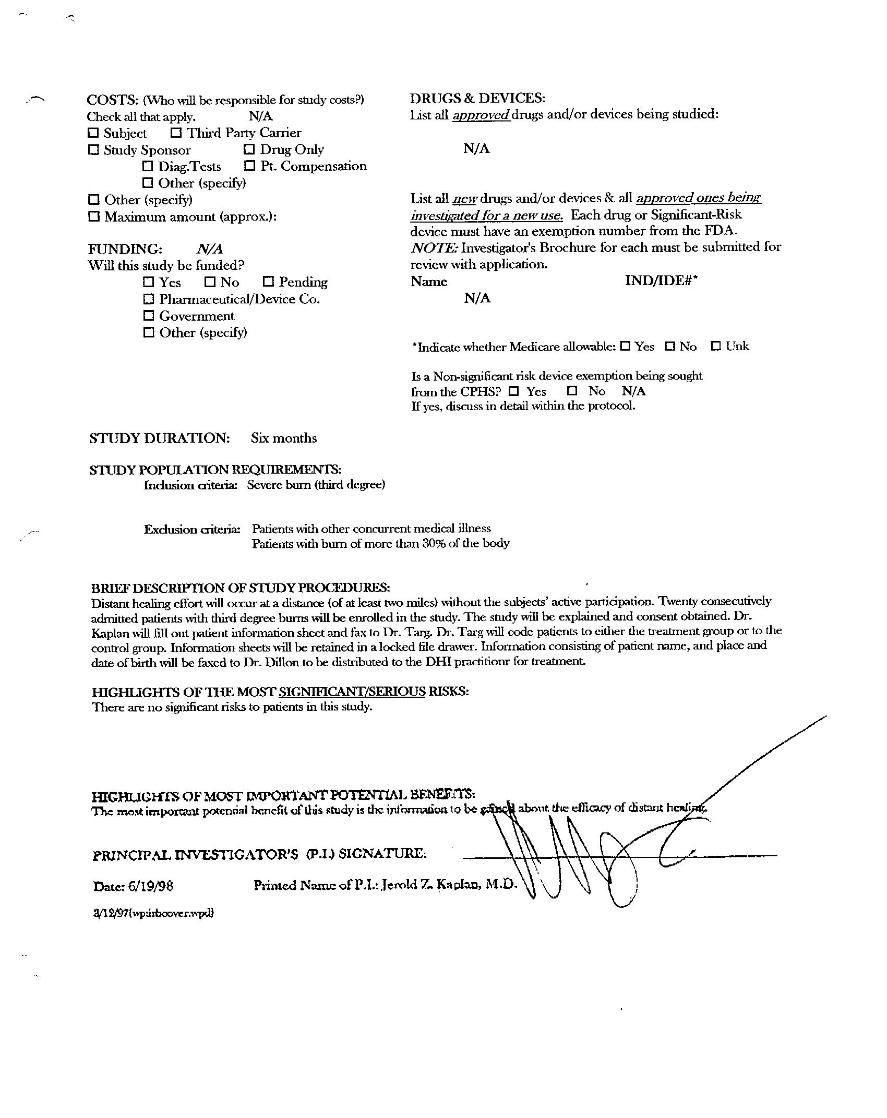
Specific design criteria for Alta Bates Burn Unit clinical trial included: Distant healing effort will occur at a distance of at least two miles without the subjects' active participation. Twenty consecutively admitted patients with third-degree burns will be enrolled in the study. Dr. Kaplan will obtain subjects' consent and explain that it is a double-blind study, therefore subjects will not know whether they are part of the treatment group or the control group. Dr. Kaplan will fill out patient information sheets and fax them to Dr. Targ. Dr. Targ will code patients to either the treatment group or to the control group. Information sheets will be retained in a locked file drawer. Information consisting of patient name, and place and date of birth will be faxed to Dr. Dillon to be distributed to the DHI practitioner (Dr. Savage) for treatment within 24 hours of burn injury. There are no significant risks to patients in this study. Purpose of the study is to test whether distant healing can effect the rate of healing of severe burns. The most important potential benefit of this study is the information to be gleaned about the efficacy of distant healing. |
Specific design criteria for Grossman Burn Unit Pilot Study included: Subjects and burn unit staff unaware of testing (with the exception of Dr. Young, Dr. Richard and Dr. Peter Grossman). . Fifteen minute SDI processing within the first four hours of burn injury. No physical contact between subjects and the SDI practitioner (located at least 10 miles from Burn Center), No interference with usual medical cares. Subject information to consist of full name, date of birth, place of birth (city and state) and time of burn. Dr. Young or burn unit staff will inform Dr. Dillon of any subject admitted with severe burns within 4 hours of injury. Dr. Dillon will distribute subject information to SDI practitioner, Dr. Philip Savage, for immediate treatment. Clinical observation of results by Dr. Young will include status of reepithelization, infection, and pain. |
| FORMAL BURN STUDY PROPOSAL TO HUMAN SUBJECTS REVIEW BOARD |

| Six-year-old Adelaide BEFORE SDI Treatment |
The extraordinary results of Dr. Savage's remote SDI intervention on Adelaide's Fire Burn were unprecedented in 2010 and have been available worldwide since then. Burn victims everywhere should be experiencing these same outcomes. To accomplish the eradication of suffering from fire burns worldwide, all it takes is the interest and cooperation of global NEWS MEDIA to report cases of fire burns and medical doctors and first-responders to verify the results of the SDI interventions. In the age of digital communication, where people all over the world have a cell phone in their pocket, there is no longer any reason for any man, woman, child or animal to ever again suffer the excruciating pain and damage of burn from fire. Dr. Savage's experiments on Fire Burn are, to date, the most important and valuable public service ever offered to humanity. The FireBurnDoctor "FREE Burns Hotline" is monitored 24/7 since 2009. |
| Six-year-old Adelaide AFTER SDI Treatment |
2. Grossman Burn Center, Sherman Oaks, California privately owned medical center in Los Angeles area |
1. Alta Bates Hospital Burn Unit, Berkeley, California, 1998-1999 sponsored by California Pacific Medical Center (CPMC), San Francisco, CA |
| Experimental Design Problem After a month of actively preparing for subjects that qualified for the Severe Burns Clinical Trial, it became very clear that the study design was not working and needed to be adjusted. The major obstacle was discovered when Dr. Kaplan was not notified at the time severe burn victims were admitted to the hospital. Patients were first treated by nurses at hospital emergency rooms and only later (after 24 hours) were transferred to Dr. Kaplan's burn unit where Dr. Kaplan was informed. Dr. Savage's DSNB protocol for burns requires that he be given burn victim coordinates as soon as the burn injury occurs and never more than 24 hours from the time of the burn. When it became clear that Dr. Kaplan would not be able to receive patients' information within 24 hours of injury, burn project coordinator, Dr. Jane Dillon, set up an interim Pilot Study at another California burn center while waiting for resolution of the obstacle at the Alta Bates Burn Unit. |
| EXTRAORDINARY RESULTS |
| | | | | | | | | |